
Spaces for diagnosis
Picture yourself in a big cathedral. All the hard surfaces of the space make the sound bounce back and forth – and you feel the energy of the sound without hearing exactly what is said just a few meters away. This is in many cases the exact same situation you have in spaces for diagnosis.
Spaces for diagnosis
Radiology rooms, MRI-centers, ultrasound, hybrid operation theatres etc. are often a challenge in regards to the sound environment. Of course the rooms have to be safe for the surrounding facilities and are therefore often built with concrete, lead and metal – i.e. hard surfaces only. Like a cathedral. Offsite construction modules are also one of the upcoming trends giving the opportunity for specialized companies to deliver a thought-through construction to fit into the hospital as a LEGO bite.
Unfortunately, these modules and diagnosis facilities are often built without thinking about the sound environment. The hard surfaces don’t support communication and staff can be very challenged in regards to both work performance and wellbeing.
A successful story: Acoustic comfort and high hygiene requirements at the Sundsvall Regional Hospital
 In Sweden, in Sundsvall Regional Hospital – a new surgical center was to be built since the existing department was opened in the mid-1970s. The premises were in disrepair and could not meet modern demands for accessibility, hygiene and working environment. Many of the installations had also reached the end of their technical lifespan. Because of this knowledge a preliminary study was carried out to draw up new proposals for a Surgical Centre that would allow premises to be updated and equipment brought up to a standard that would safeguard its performance for many years. Seventeen operating rooms required renovation and 14 new rooms would be added, including a new, 105-square-metre hybrid operating room – with the possibility of doing both X-ray, ultrasound, MRI scanning.
In Sweden, in Sundsvall Regional Hospital – a new surgical center was to be built since the existing department was opened in the mid-1970s. The premises were in disrepair and could not meet modern demands for accessibility, hygiene and working environment. Many of the installations had also reached the end of their technical lifespan. Because of this knowledge a preliminary study was carried out to draw up new proposals for a Surgical Centre that would allow premises to be updated and equipment brought up to a standard that would safeguard its performance for many years. Seventeen operating rooms required renovation and 14 new rooms would be added, including a new, 105-square-metre hybrid operating room – with the possibility of doing both X-ray, ultrasound, MRI scanning.
Unfortunately, the planned package solution for the operating and diagnosis rooms, based on a modular solution, didn’t meet the room acoustic demands of the Swedish standard. Floors, walls and ceilings adversely affected the sound environment and the absorption of sound was more or less non-existent in the solution. This was due to the module material properties of glass and metal, which instead of decreasing the reverberation time instead contributed to increase it.
Reverberation time according to the Swedish standard (SS25268)

Reverberation time in these facilities, according to the Swedish standard (SS25268), cannot exceed 0.6 sec. and calculations on the hybrid operation theatre showed values over 2 seconds! Again think about the cathedral – and now think that you have to communicate clearly around critical ill patients – trying to compete with the sounds of the technical equipment. In specialists’ areas like these it is not unusual to have a lot of sound sources and peak levels can reach more than 100 dB [1].
In the above Swedish case the project group decided to change the metal ceiling into an acoustic ceiling (absorbing tiles meeting absorption class A [2] according to ISO 354, ISO 11654). They chose a ceiling that also met the hygiene demands in regards to cleaning and disinfection. Acoustic measurements were done according to ISO 3382 and after changing the ceilings – the facilities met the acoustic demands which means that the reverberation time was halved!
Reverberation time and other room acoustic parameters
So what does it mean - Half the reverberation time?
Reverberation time is defined in ISO 3382-1 as the time it takes for sound source to decrease in level by 60 dB after the source emission has stopped. Reverberation time is more commonly measured, for practical reasons, over a 20 or 30 dB decay (T20 and T30) starting 5 dB below the initial level and then extrapolated to the full 60 dB range.
In short, reverberation time tells us something about how long sounds remain in the room before they disappear; and because of the different energy in speech sounds – consonants and vowels, communication can be blurred and noise will build up when the reverberation time is too long.
In our vowels we have lot of energy (when we pronounce our vowels – nothing inhibits the sound on its way out) in comparison to the energy of our consonants that is limited because of obstructing the airflow (pronouncing e.g. the sound ‘k’) or by constricting the vocal tract, causing friction as the air passes through it (pronouncing e.g. the sound ‘f’).
When we add long reverberation time to speech the vowels will therefore take over because they have much more energy from the beginning – and the speech will be blurred. When we can’t hear or understand speech we raise our voice to be heard and then the sound builds up. This is called the Lombard effect. So when we go from long reverberation time (e.g. 2 sec. in the aforementioned Swedish hospital) to short reverberation time (0.6 sec.) – we make speech more clear.
Together with this the sound pressure levels go down in general and create a calmer sound environment, which facilitates not just the more effective and efficient transmission of information but also enables acoustic comfort amid staff and patients.
How do we experience changes in reverberation time?
Even small changes in reverberation time will have an effect on staff (the just noticeable difference – JND – according to ISO3382-1 is only 5%).
The Hvidovre Hospital
In a study in Denmark (Hvidovre Hospital) three operation rooms were altered acoustically (absorbent ceilings + wall panels) and the rooms went from 0.7 sec. to 0.6 sec. and to 0.5 sec.
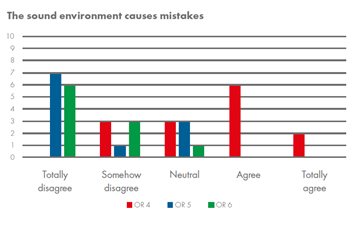
The staff members were asked questions relating to aspects like ‘the sound environment makes me tired’, ‘the sound environment causes headaches’ and ‘the sound environment makes us talk louder’.
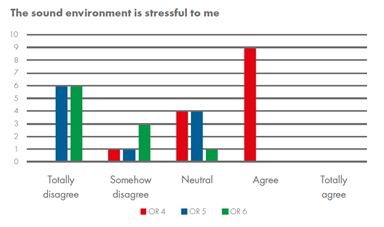 In all cases the answers followed the trend of the acoustic measurements. In OR 4 (0.7 sec.) staff were generally more disturbed and suffered because of the sound environment, in OR 5 (0.6. sec.) they were more positive and in OR 6 (0.5 sec.) they were the most pleased.
In all cases the answers followed the trend of the acoustic measurements. In OR 4 (0.7 sec.) staff were generally more disturbed and suffered because of the sound environment, in OR 5 (0.6. sec.) they were more positive and in OR 6 (0.5 sec.) they were the most pleased.
What needs to take into account to enable acoustic comfort?
Spaces for diagnosis are crucial in regards to taking the right decisions and often the patients involved are critically ill and way out of their comfort zone to be aware of what has been said when and by whom. These facilities have to support clear communication to control the risk of mistakes at the same time as they have to support wellbeing of both staff and patients.
We are all affected by sound – but in critical care we have a complex situation. Room acoustics needs to be part of a sustainable solution in healthcare in general – and building a ‘cathedral’ in regards to sound is never the way to go.
The first thing for a room of such type to be successful in terms of acoustics is to make sure that overall sound levels are kept as low as possible and consequently the reverberation time is not too high and the previously mentioned Lombard effect does not come into play.
The latter can be done through installing a wall-to-wall class A absorbing ceiling. In order to further support the information transmission (i.e. to improve the so-called acoustic parameter speech clarity), wall panels in adjacent perpendicular walls can be hang so that grazing waves bouncing back and forth parallel to the floor and ceiling are reduced markedly. In all these acoustic solutions, it should not be forgotten that not only acoustic but also hygiene requirements should be fulfilled.
All in all, we should keep in mind that acoustics is a key factor for the activities taking place inside spaces devoted to diagnose inside hospitals (as well as in many others) and should therefore not be forgotten in their design if successful spaces are to be built.
References
NB. This article was originally published in Spanish at www.hospitecnia.com. Find the article here.
SS 25268:2007. Acoustics – Sound classification of spaces in buildings – Institutional premises, rooms for education, preschools and leisure-time centres, rooms for office work and hotels (in Swedish), Swedish Standards Institute, Stockholm, Sweden.
ISO 354:2013. Acoustics – Measurement of sound absorption in a reverberation room, International Organization for Standardization, Geneva, Switzerland.
ISO 11654:1997. Acoustics – Sound absorbers for use in buildings–Rating of sound absorption, International Organization for Standardization, Geneva, Switzerland.
ISO 3382-1:2009. Acoustics – Measurement of room acoustic parameters – Part 1: Performance spaces, Organization for Standardization, Geneva, Switzerland.
[1] As a matter of comparison, sound levels in a library are of around 35-40 dB, a conversation at normal volume at 1 m distance from the talker amounts around 60 dB, and an airplane taking off next to us would produce around 120 dB.
[2] Absorption is the ability of a material to convert sound energy into heat, i.e. to not send back to the room reflected sound once it impinges against its surface. In broad strokes, one can say that the absorption coefficient indicates the percentage of energy which remains inside the material respect the total incident energy. It is denoted by the Greek letter alpha α which ranges between 0 (a total reflective material) and 1 (total absorption). A class A absorption material has an αw ranging between 0.9 and 1 (weighted average value, as absorption depends on the frequency).